DIAGNOSES & TREATMENT
UTERINE FIBROIDS
Just as there are a variety of types of uterine fibroids, there are a range of treatment options. Explore the symptom and treatment options below – including the benefits of the minimally invasive laparoscopic approach to uterine fibroid treatment.
Uterine fibroids aka fibroid tumors are benign (non cancerous) growths that occur within the smooth muscle of the uterus called the myometrium. Typically, uterine fibroids are slow growing, benign tumors and are most commonly found in women during the ages of 25-50. The malignant or cancerous form of a fibroid tumor is called a leiomyosarcoma, this type of tumor is very, very rare.
Uterine fibroids are the most common cause of hysterectomy (uterus removal) in the United States. However most women do not need their uterus removed and instead can have an alternative treatments such as a myomectomy which means removing the tumor from the uterus.
70-80% of women have uterine fibroids, however not all are symptomatic or require treatment.
Uterine Fibroid Symptoms:
- Heavy vaginal bleeding
- Irregular menstrual cycles
- Anemia (low blood count)
- Pelvic pain
- Pelvic or vaginal pressure
- Abdominal cramping
- Abdominal distention
Causes of Uterine Fibroids:
While the specific cause of uterine fibroids is unknown, we do know that they respond to hormones such as estrogen and progesterone and grow during the reproductive years. Fibroids seem to start to growing in women between ages 25 and 35. Once a woman goes into menopauses (average age of 51) the fibroids typically shrink and women will often stop having symptoms.
African-American women have a higher risks of fibroids compared to Caucasian women and women that have mothers or sisters with fibroids have a higher risk of having them as well. Pregnancy and childbirth seem to decrease the risk and many fibroids do shrink once a woman reaches her menopausal years. It is thought that estrogen increases the growth of fibroids; therefore if a woman utilizes post-menopausal hormone replacement with estrogen, the fibroids may not shrink as much as they would otherwise.
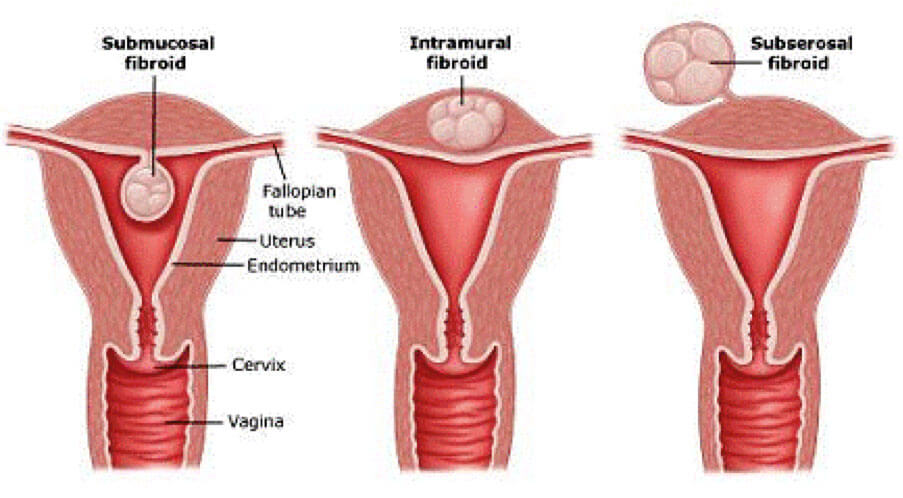
Types of Uterine Fibroids:
The location of the fibroid in or on the uterus will determine the type of uterine fibroids.
- Submucosal fibroids – are fibroids that grow inside the cavity of the uterus. This type of fibroids is typically treated with hysteroscopic (a camera inside the uterus itself) resection or removal.
- Intramural fibroids – are fibroids located in the muscle layer of the uterus itself. These fibroids are most commonly treated laparoscopically.
- Subserosal fibroids – are fibroids located on the outside of the uterus (i.e. toward the abdominal side of the uterus). These are the ones that are typically treated through laparoscopy.
Diagnosis of Fibroids
Ultrasound or MRI of the uterus is the best way to diagnose the location, number and type of fibroids as well as the overall size of the uterus.
Dr. Moore and Dr. Miklos have been performing laparoscopic myomectomy for over 20 years.
Drs. Miklos & Moore are considered worldwide EXPERTS in Laparoscopic Approach to Advanced Gynecologic Surgery including Laparoscopic Myomectomy.
- Hysterectomy (uterus removal) – is the most common treatment in the USA today. It is typically NOT necessary to remove the uterus to treat symptoms of fibroids.
- Myomectomy – removing the individual fibroid tumor while preserving the uterus
- Laparoscopic Myomectomy – removing the fibroid tumors using a miniature incision approach through the abdomen.
- Robotic Myomectomy (Robot assisted laparoscopic surgery, typically robot not necessary and much more expensive)
- ExAblate (MRI focused Ultrasound Ablation of Uterine Fibroids)
Laparoscopic Approach Benefits:
- Less Pain
- Small scars
- Smaller incisions than robotic surgery
- Faster recovery
- No hysterectomy
Laparoscopic myomectomy is completed by inserting a small camera through a tiny incision in the belly button and working off High-Definition Video monitors to surgically remove the fibroids.
Once the fibroids or myoma’s are visualized and injected with a vasoconstrictive agent such as Pitressin solution. This decreases the blood flow to the fibroid and allows the removal of the fibroid(s) from the uterus with minimal bleeding.
Laparoscopic surgery for uterine fibroids can be complex in nature and does require a high-level of surgical expertise for a successful outcome. Drs. Moore and Miklos can complete a laparoscopic fibroid removal with precision and minimal bleeding.
Laparoscopic suturing of the
uterine defect
Once laparoscopic fibroid removal is completed the defect in the uterus must be closed. This is the step that is rate limiting for many surgeons, they do not have the skill to put in sutures laparascopically. i.e. Suturing laparoscopically is one of the most difficult skills to master.
Robot vs. Laparoscopic Approach
“The Robot” has been introduced to help surgeons with the difficult skill of suturing however in skilled surgeons hands the robot is not necessary. Robotic Surgery has been shown to cause more post-operative pain, take much longer than traditional laparoscopic surgery (therefore longer anesthesia), utilize more and larger incisions, and cost significantly more than laparoscopic surgery while offering no benefit.
Removing the Fibroids WITHOUT a Power Morcellator
Recently, concern has been raised regarding “power morcellation” of the fibroids once they have been removed from the uterus. Typically, the fibroid tumors are too large to remove from the small laparoscopic incisions and therefore have to be reduced in size. Power morcellators are electric or battery powered devices, which cut up the fibroids into small pieces so they can be easily removed through the small abdominal incisions. Many patients are concerned that the use of a power morcellator may potentially spread any unrecognized uterine cancer cells. Drs. Miklos & Moore do not use power morcellators in fibroid removal.
Complications and Recovery
Laparoscopic Myomectomy has risks similar to other laparoscopic pelvic surgery including:
- Bleeding requiring transfusion (< 1% risk)
- Ureter or bladder injury (< 1% chance)
- Bowel injury (< 1%)
- Continued uterine bleeding or pain
- Recurrence of fibroids
- Post operative adhesions
Recovery times for laparoscopic myomectomy vary, however typically patients are able to resume normal daily activities in 7 to 10 days and sometimes in as little as 2 to 3 days.