DIAGNOSES & TREATMENTS
URINARY INCONTINENCE, SLING PROCEDURES & NON-MESH TREATMENT OPTIONS
Treating female urinary incontinence safely and effectively is a top priority for Drs. Miklos & Moore. Here you will find an overview of the diagnosis of urinary incontinence and the procedures available.
Diagnosis:
• Urinary Incontinence
Treatments:
• Laparoscopic Burch (A NON-MESH surgical treatment)
• TVT Sling
• TOT Sling
• Single Incision Sling
Diagnosis
URINARY INCONTINENCE
Female urinary incontinence (urinary leakage) refers to the involuntary loss of urine from the bladder. It can be a cause of anxiety, social embarrassment and may limit ones social and daily activities. Fortunately most conditions of urinary incontinence can be successfully managed.
There are two main types of urinary incontinence:
1) Urgency (Overactive Bladder) – is most often described as having difficulty maintaining ones urine on the way to the restroom. Patients usually describe frequency, urgency of urination as well as nighttime urination. Urgency incontinence is usually treated with medication.
2) Stress Urinary Incontinence (cough or activity related) – is most often described as loss of urine during coughing, sneezing, laughing or with other physical activities such as running, jumping, exercise etc. This type of incontinence is most commonly treated with a Burch or sling procedure. These two surgeries focus on urethral suspension and not bladder support. Supporting the urethra is the best way to stop stress urinary leakage.
Treatments
• Laparoscopic Burch (A NON-MESH surgical treatment)
• TVT Sling
• TOT Sling
• Single Incision Sling
Laparoscopic Burch Procedure
Non-Mesh Surgery for Incontinence (SUI)
The Burch procedure has remained one of the top 2 curative surgeries in the treatment of stress urinary incontinence since the early 1960’s. The Burch procedure uses sutures to stop stress urine leakage and has become a popular alternative to operations using mesh (i.e. TVT, TOT and single incision slings). Instead of using a synthetic mesh to lift up the urethra the Burch procedure uses sutures to lift the patient’s own vagina to elevate the urethra. The laparoscopic Burch cure rates are equivalent to the cure rates of slings.
Laparoscopic Burch Procedure:
- Miniature incisions
- < 30 minute procedure
- 1 day hospital
- Cure Rate – 90%
Laparoscopic Burch Complications:
- Bladder injury < 1%
- Urethra injury < 1%
- Urter injury < 1%
- Urine retention 1%
The laparoscopic Burch is performed through miniature incisions on the abdomen and usually takes less than 30 minutes to perform. Once inside the abdomen the surgeon explores the area above the ceiling of the vagina. The surgeons places 4 sutures through the vagina wall and then anchors these sutures to the Coopers ligaments on the pelvic bone and stops the loss of urine leakage with activity 90% of the time.
Drs. Miklos & Moore have been performing laparoscopic Burch procedures since 1993 and have performed more than 800 of these procedures. Many patients are told this operation is not successful or it has low cure rates when in fact this is not true. Many surgeons will tell their patients this simply because they cannot perform a laparoscopic Burch as the procedure is technically challenging.
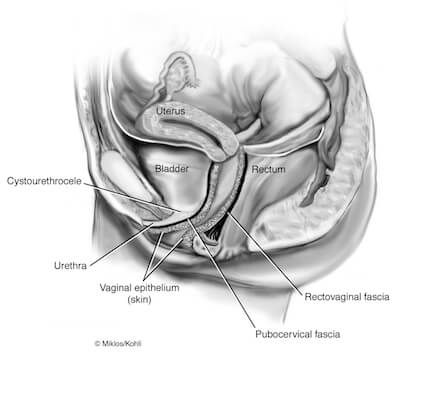
Sagging Urethra (side view)
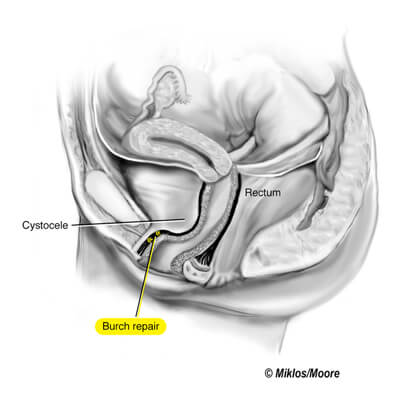
Supported Urethra after a Burch (side view)
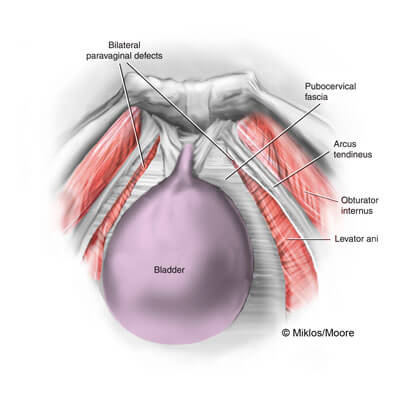
Sagging Urethra & Bladder
(birdseye view)
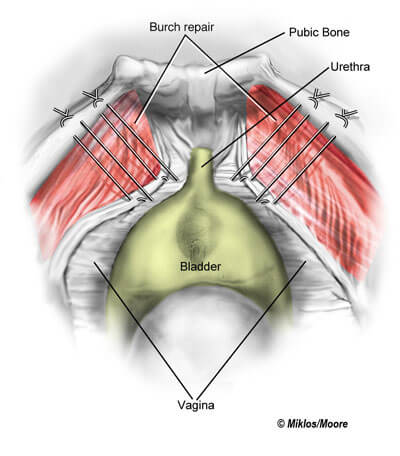
Supported Urethra after Burch
(birdseye view)
Tension-Free Vaginal Tape (TVT) Sling
The TVT sling was developed in Sweden in 1994 and released in the USA in 1998. Dr. Miklos was one of the first 5 surgeons in the USA to use and teach the technique. The technique is considered to be the “gold standard” surgery in the treatment of stress urinary incontinence by urogynecologists and urologists alike. The procedure is performed starting with the placement of the sling through an incision in the vagina and then exiting the pelvis through two small incisions at the pubic hairline.
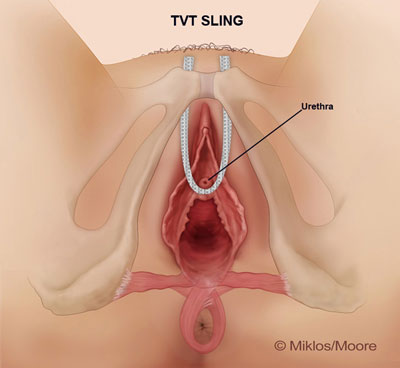
TVT Sling
- 20 minute procedure
- 90% cured in 1st year
- 85% cured in 5th year
- 1-2% urine retention
- Less than a 1% blood transfusion rate
Transobturator (TOT) Sling
The TOT sling made its debut in Belgium and France in 2001. It was considered the second-generation synthetic mesh sling. This device, like the first generation TVT sling, is also placed through a vaginal incision underneath the urethra but it exits the pelvis through small groin incisions. Though this sling initially showed promise with cure rates equivalent to the TVT sling and the Burch procedure, Drs. Miklos & Moore no longer offer this technique except for rare and unusual cases.
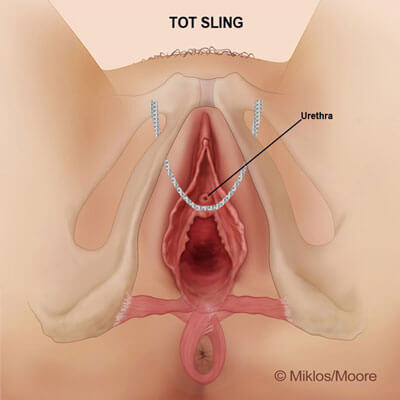
TOT Sling
- Minimally invasive
- 85% cure rate in 1st year
- 90% cure rate in 5th years
- Potential for severe groin pain
- Potential for severe leg pain
Single Incision Slings
Mini Sling
The Single Incision Sling (SIS) is a smaller sling delivered through a single incision site underneath the urethra just like the TVT and TOT sling. Unlike the TVT and TOT slings that require 3 incisions, the SIS requires just one small ¾ inch incision. The mini sling was produced in an attempt to maintain cure rates for stress urinary incontinence yet reduce complications.

Single Incision Slings
- 1 incision
- 5 to10 minute procedure
- Cure rate 90% at 1 year
- Less post operative pain