
Failed mesh removal Yale University Hospital.
This patient is a 41-year-old woman from Danbury, CT who had a TOT sling (Figure 1) for stress urinary incontinence (2014). The sling was too tight and she had it revised for incomplete bladder emptying. (Figure 2) (2017) The same urogynecologist then placed a TVT retropubic sling (Figure 3) for recurrent stress urinary incontinence (2017). As of 2017 she has both a TOT and a TVT sling.
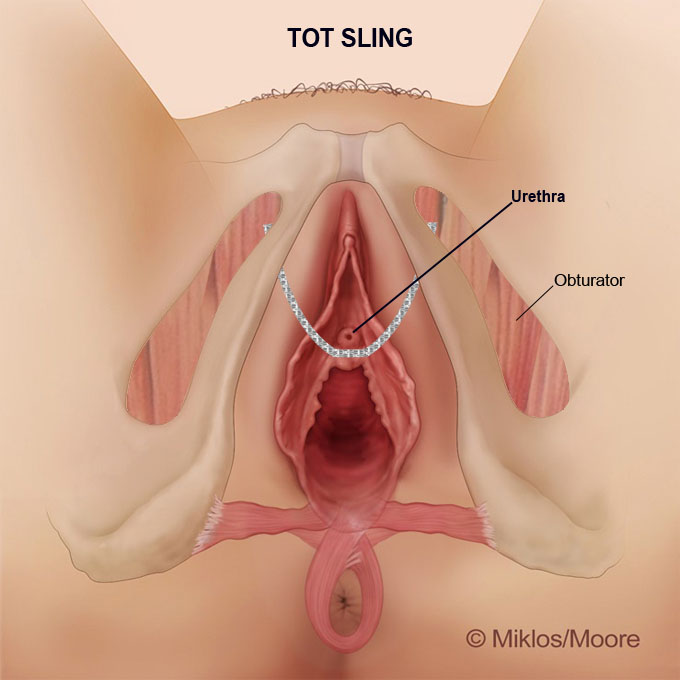
Figure 1: TOT Placement
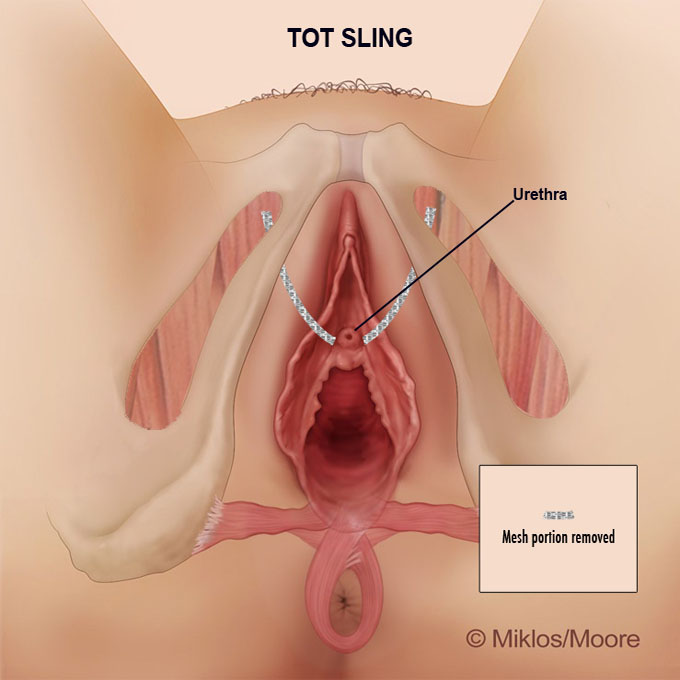
Figure 2: TOT Revision
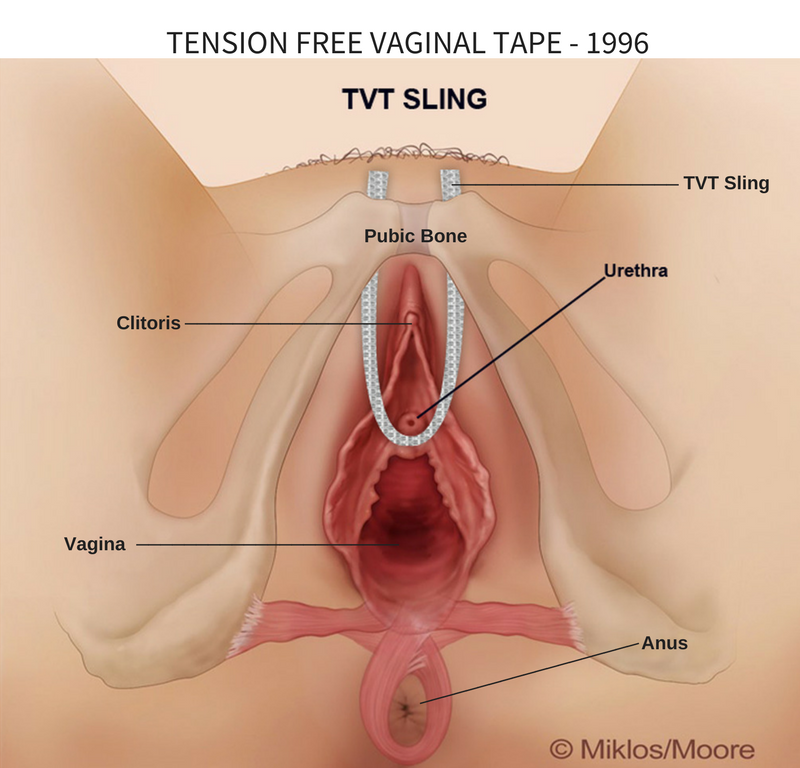
Figure 3: TVT Placement
This patient complained of severe pain immediately after the TVT sling placement. Her urogynecologist told her that nothing could be done to help her so the patient sought treatment at Yale University Hospital where she saw a female urology specialist. This urologist told her THE MESH COULD NOT BE REMOVED but did offer: 1) trigger point injections 2) medical therapy with gabapentin and 3) physical therapy (PT). The patient did all three therapies and explained she could only tolerate 2 weeks of PT because it made her pain worse.
The patient finally saw a urologist who is well trained in Urogynecology in Connecticut and tried to revise the sling (i.e. by trimming) and then she had a second surgery by this doctor who then removed approximately 2.5 cm of mesh from underneath the skin inside of the vagina. (2018) This did not help her pain. She now suffers from stress urinary incontinence again.
The patient found Drs. Miklos & Moore in Atlanta, Georgia and described that she was having left lower abdomen and “pubic area” pain which radiated to the groin. An evaluation revealed it was not radiating to the area of the groin where the TOT sling was placed. Using this information and the fact that the patient did not get lower abdominal and pubic pain until after the TVT sling placement, Dr. Miklos recommended only the removal of the TVT sling. He thought based upon her exam and history that the TOT was the problem.
Dr. Miklos performed a 2-cm vaginal incision and laparoscopic incisions (Figure 4) to remove the TVT sling. (NOTE: TVT slings cannot be completely removed through only a vaginal incision, this is not possible). Most patients get approximately 20 cm of mesh when they get a TVT placed. When a TVT is placed for stress urinary incontinence it is placed without visualizing the inside of the body, but if placed correctly this is where the sling should be inside of the body. (Figure 5a and 5b)
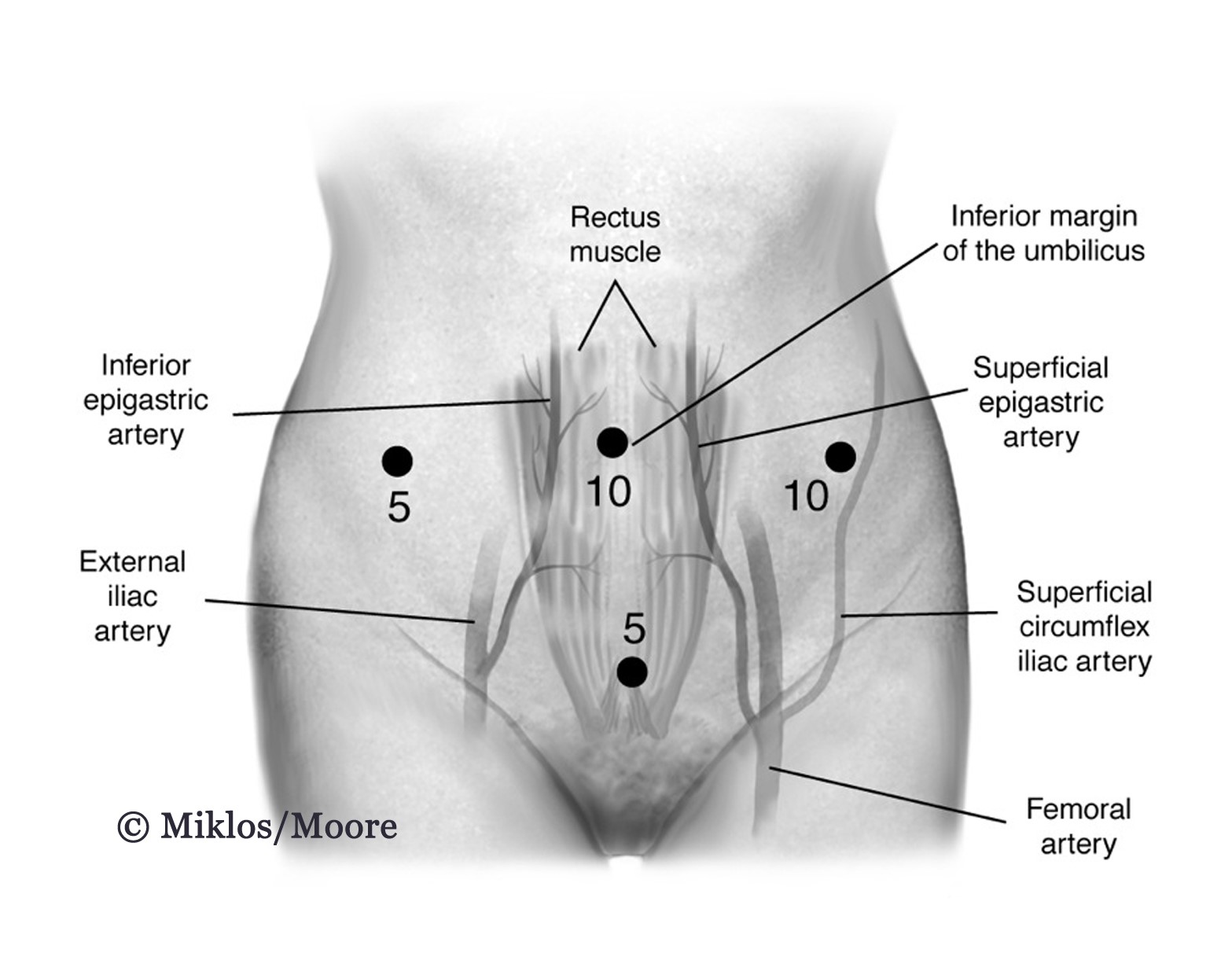
Figure 4: Laparoscopic Incisions
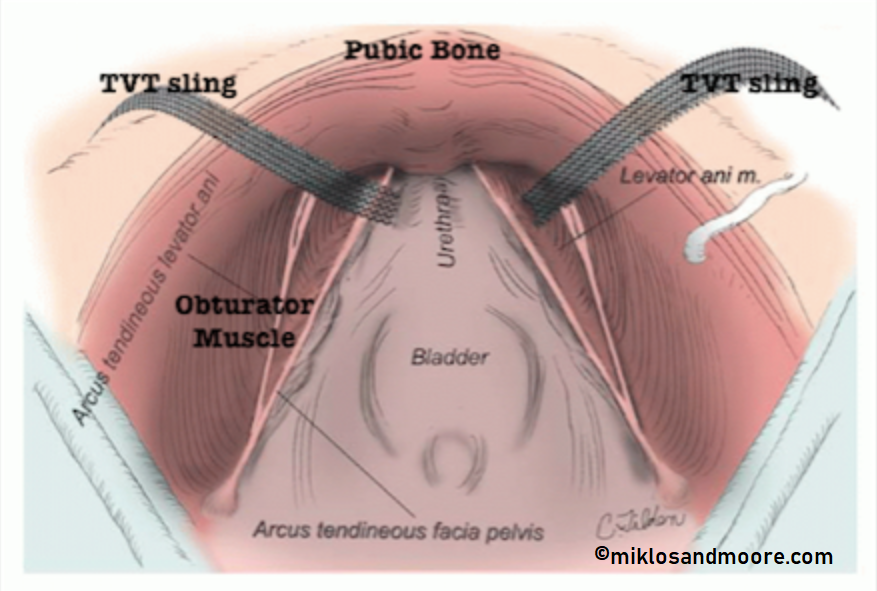
Figure 5A: illustration of normal TVT placement in pre-pubic space
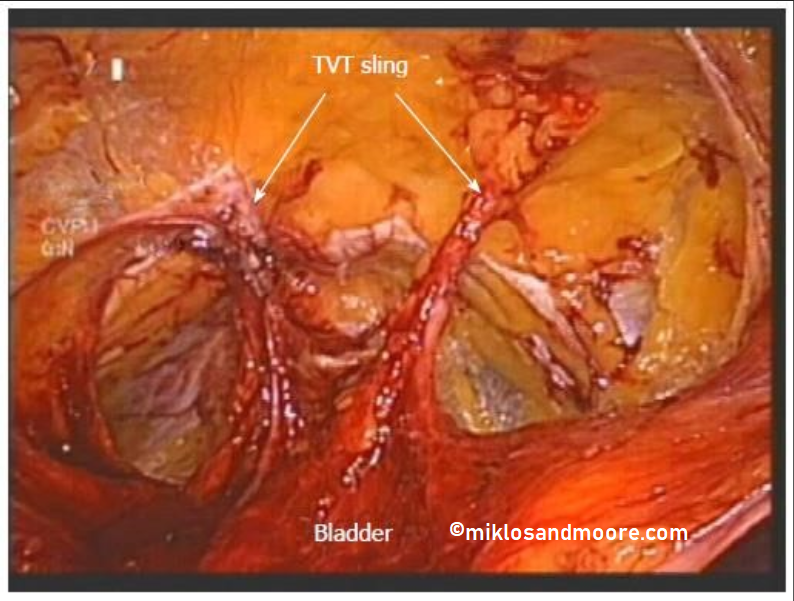
Figure 5B: picture of normal TVT placement in pre-pubic space
When Drs. Miklos & Moore entered the pre-pubic space, this is not where they found the mesh, instead the mesh was very much out of position with ½ of the mesh not inside of the pre-pubic space but instead buried into the obturator internus muscle. (Figure 6) Please note: in this photo there is no mesh below the pubic bone, it is buried behind the obturator internus muscle – this photo is an example of another patient with the same problem but on the right side.
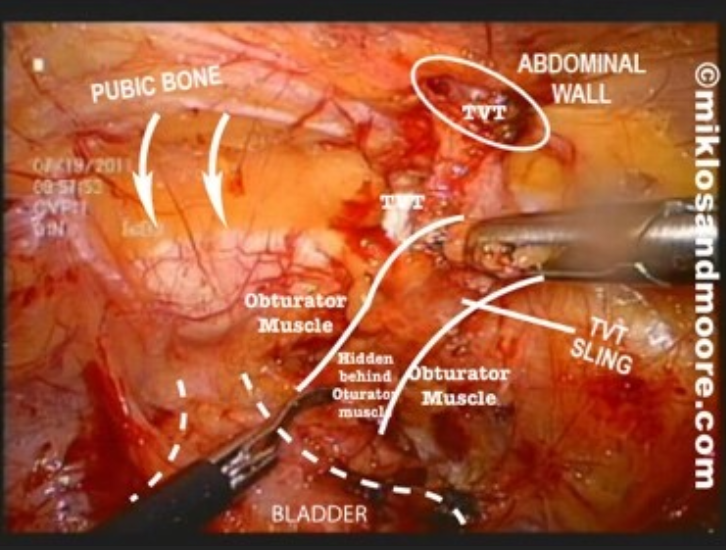
Figure 6: example of TVT beneath muscle)
Our patient had her mesh buried beneath the obturator internus muscle on the left side and this figure shows the mesh almost completely dissected out of the muscle. (Figure 7) This final figure shows the complete mesh removal of over 24 cm of mesh, the other structure is an IUD which the patient wanted removed at the time of surgery. (Figure 8)
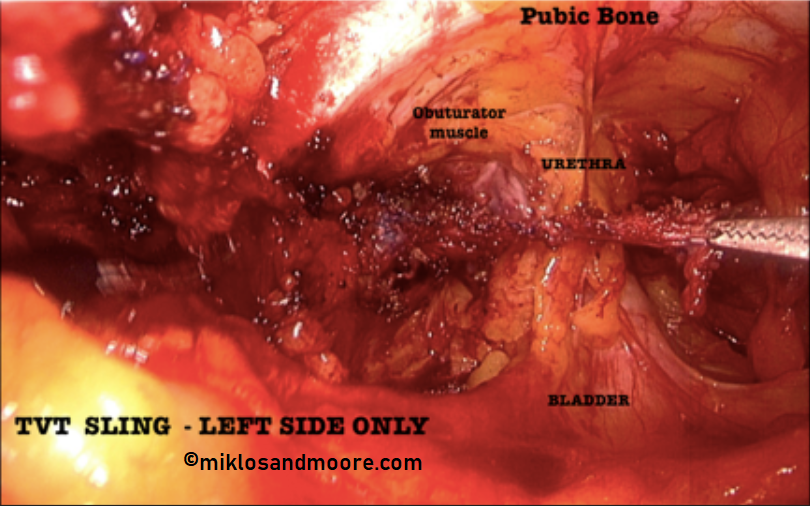
Figure 7: TVT Removal – Left Side
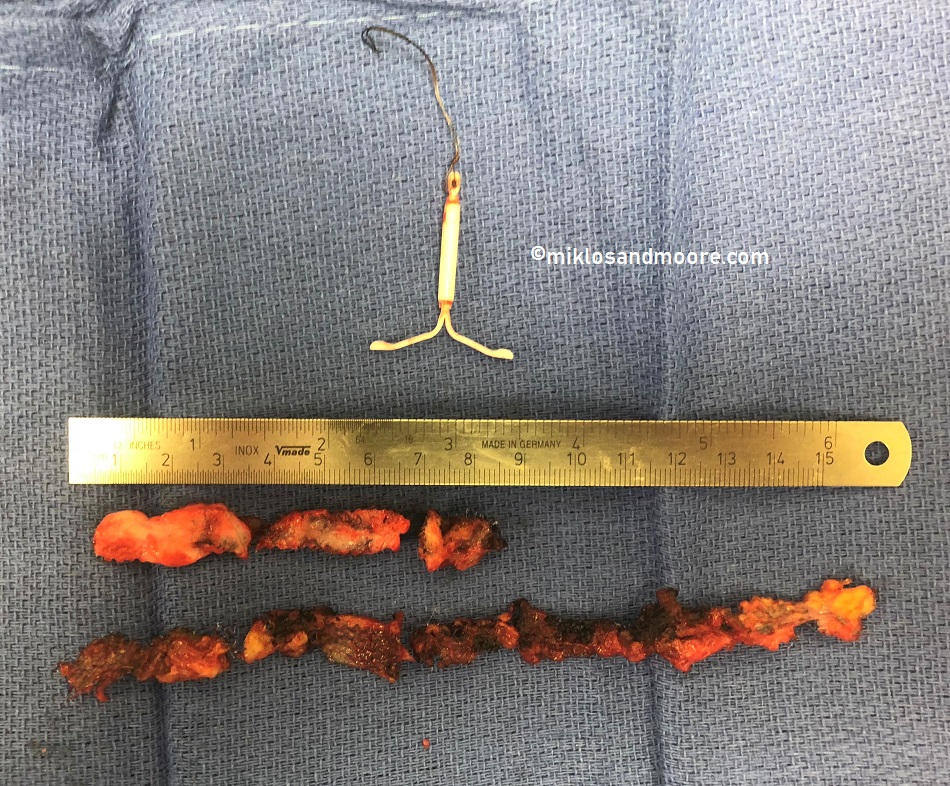
Figure 8: TVT Sling Removed (24 cm = 10 inches)
Drs. Miklos & Moore Pearls of Wisdom:
- Patients with vaginal pain can only have the vaginal portion of the TVT or TOT sling removed, but a minimal of 5-6 cm should be removed and not just cutting the sling.
- If a patient has lower abdominal pain and vaginal pain then the whole sling should be removed (average length is 14-24 cm).
- It is impossible to remove the whole TVT sling from a vaginal approach alone. Any surgeon who tells you that the whole TVT can be removed through a vaginal incision is either ignorant or not being truthful.