Prolapse vs Vaginal Laxity: How to Tell the Difference
Prolapse vs Vaginal Laxity: How to Tell the Difference (Symptoms, Causes, and Treatment)
Many women are told they have “vaginal laxity” when something feels off—but in reality, they may have pelvic organ prolapse, a completely different condition that requires a different type of treatment.
Understanding the difference is critical, because:
Treating the wrong condition leads to poor outcomes, persistent symptoms, and unnecessary procedures
Why This Confusion Happens
Both conditions can occur:
- After childbirth
- With aging
- With pelvic floor changes
Both may cause:
- A “different” or “looser” feeling
- Changes in sexual function
But beneath the surface, they are fundamentally different.
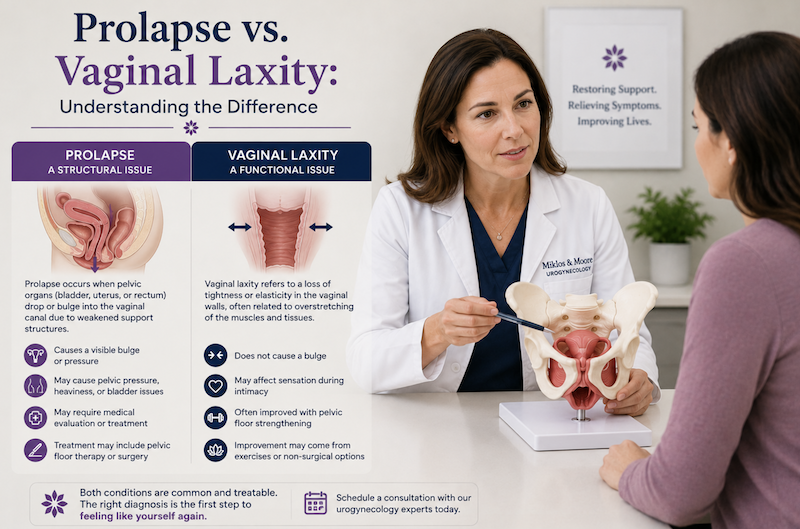
What Is Vaginal Laxity?
Vaginal laxity refers to a loss of tightness or tone in the vaginal tissues.
Causes:
- Vaginal childbirth
- Stretching of tissue
- Reduced collagen and elasticity
- Muscle relaxation due to nerve damage
Symptoms:
- Feeling of looseness
- Decreased friction during intercourse
- Reduced sensation during intercourse
The patient can have minimal or little structural descent of organs known as prolapse.
What Is Pelvic Organ Prolapse?
Pelvic organ prolapse is a structural condition where pelvic organs descend due to weakened support.
This may involve:
- Bladder
- Rectum
- Uterus
- Urethra
The Key Differences (Most Important Section)
| Feature | Prolapse | Vaginal Laxity |
| Bulge | ✅ | ❌ |
| Pelvic pressure | ✅ | ❌ |
| Worse standing | ✅ | ❌ |
| Loose feeling | ⚠️ sometimes | ✅ |
| Deep pain with sex | ✅ | ❌ |
| Organ descent | ✅ | ❌ |
This distinction is critical for correct diagnosis. The patient with only vaginal laxity will often have minimal prolapse, but those with prolapse have a high incidence of vaginal laxity.
What Patients Actually Experience
Vaginal Laxity:
- “It feels looser”
- “Less sensation during sex”
Prolapse:
- “Something is falling out”
- “There’s pressure or heaviness”
- “I feel a bulge”
Why Misdiagnosis Happens So Often
Many providers:
- Focus only on the signs of prolapse during the exam and not the symptoms
- Use a full metal or plastic speculum when inserted into the vagina pushes all the bulges back into place making them difficult to see during the exam.
- Do not perform full structural evaluation which is best done with a ½ of a speculum
- Do not ask the patient and listen to the patient about her underlying problems and symptoms
Why Non-Surgical Tightening Procedures Don’t Fix Prolapse
Procedures such as Mona Lisa, Morpheus, Radiofrequency, Microneedling, PRP, Laser therapy
- Address the skin and its collagen production
- Do not address the deeper muscle tissue
- Improve skin tone
- May enhance sensation
But they do NOT:
- Lift adequately lift organs
- Restore support structural support only skin support
- Correct structural defects
This is why surgery is often a better long term solution to vaginal laxity
Can You Have Both at the Same Time?
Yes.
Most patients have:
- Structural prolapse
- AND tissue laxity
These cases require comprehensive treatment planning
How the Right Diagnosis Is Made
A proper evaluation includes:
- Physical examination
- Identification of all compartments
- Symptom correlation
- Listening to the patient
Why Expertise Matters
Specialists like Miklos and Moore Urogynecology focus on:
- Differentiating structural vs skin tissue issues
- Identifying multi-compartment prolapse
- Preserving sexual function
- Avoiding unnecessary procedures
Treatment Differences
Vaginal Laxity:
- Pelvic floor therapy
- Energy-based treatments (selected cases)
- Surgical tightening
Prolapse:
- Pessary
- Reconstructive surgery
- Hysteropexy
A Critical Insight
If you feel:
- A bulge
- Pressure
- Symptoms that worsen standing
It is far more likely to be prolapse—not laxity
Final Takeaway
These conditions are often confused—but they are not the same.
Correct diagnosis is the difference between:
- Temporary improvement
- And lasting resolution