
What is a neovagina?
A vagina canal is usually created or lengthened through a surgical procedure. A neovagina can also be created by stretching of the patients’ vaginal skin using dilators.
Indications for a neovagina?
The most common indication for a neovagina in women is vaginal agenesis. Vaginal agenesis is a rare disorder in which the vagina doesn’t develop, and the womb (uterus) may only develop partially or not at all. Thus, patients may have only a short vagina or a vagina of minimal length. Naturally occurring short vaginas are most commonly due to medical conditions such as MRKH (Mayer-Rokitansky-Kuster-Hauser, Bardet- Biedl, Fraser Syndrome, or AIS (Androgen Insensitivity) syndrome.
Other diagnoses which are indications for a neovagina include surgically shortened vaginas and patients who have pain at the vaginal vault (aka cuff or apex) with intercourse or palpation. Patients who have surgically shortened vaginas or vaginal vault pain most commonly have had a hysterectomy.
Are there various Neovagina surgical techniques?
There are many different types of surgical neovaginas, including, but not limited to:
- Davydov Procedure (Peritoneal Pull-Through)
- Vecchietti Procedure
- McIndoe Vaginoplasty
- Colon or Bowel Neovagina
- Gracilis Flap Procedure
The Davydov (peritoneal pull through) Neovagina procedure is Dr Miklos & Moore operation of choice as it is minimally invasive (i.e., laparoscopic/robotic) with a very high success rate and a low complication rate. The surgery can usually be performed in less than 2 hours resulting in a full-length vagina (10-13 cm) 99% of the time. Dr Miklos & Moore have performed the Davydov, Vecchietti and McIndoe procedures in the past but have chosen the Davydov due to its very high success rate, minimally invasive technique, minimal blood loss and complication rate.
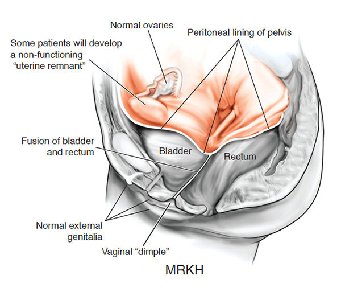
MRKH patient – no vagina
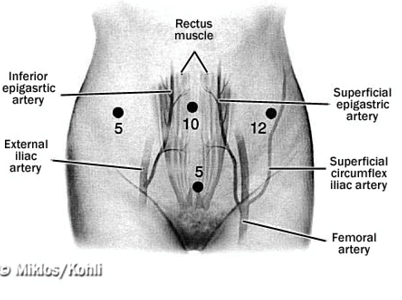
Laparoscopic incision sites for Davydov Neovagina
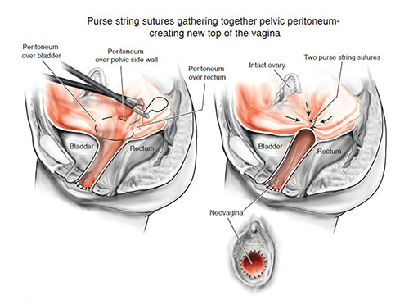
MRKH patient – after Davydov Neovagina
The Vecchietti Procedure utilizes an acrylic olive shape apparatus that is applied under tension (via threads that are brought up through the abdominal wall via incision in the abdomen) against the vaginal dimple. A large metal traction device remains on the abdomen and is then used on the threads on the abdominal wall and tightened over time that draws the olive upward and stretches the skin, thus creating a neovagina. This can take up to 3 months to accomplish.
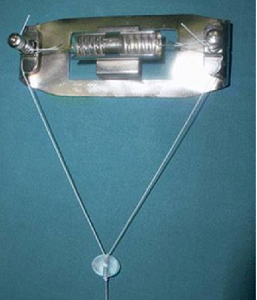
Vecchietti Neovagina – tension plate and retraction olive to stretch vagina
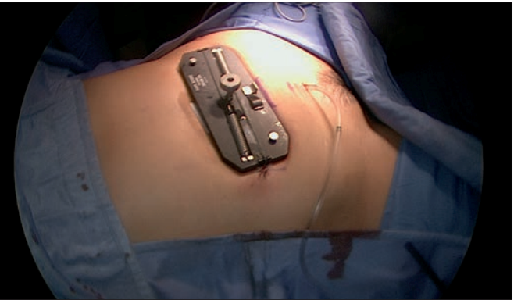
Vecchietti Neovagina- tension plate on abdomen after the surgery 2-3 weeks
The McIndoe is a less complicated procedure which is performed through the vaginal opening and requires skin grafts and/or muscle grafts from the thigh or leg. This procedure requires a constant implant in the vagina for up to 3 months after surgery to maintain the vaginal caliber. It has a much lower rate of success than the Dayvdov procedure.
Bowel Vaginoplasty uses the sigmoid colon or other loop of intestinal bowel can be transposed down into the pelvis and utilized as a new vagina. This requires the bowel / intestines to be cut and a portion removed and then utilized to make the vaginal canal. This is a major abdominal surgery that requires bowel resection and carries major risks and complications. Though the surgery can give an adequate vaginal length, patients often complain of the malodorous discharge ( a fecal odor) of the vagina after the surgery.
Gracilis Flap neovagina require large scars on the inner thigh and then a transposition of the large inner thigh muscle to make the vaginal canal. This surgery is often extremely disfiguring and has a propensity to scar down and patients often complain of hair growth inside of the vagina after surgery
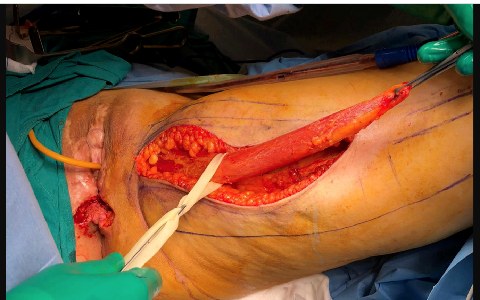
Gracilis Neovagina – muscle harvesting

Gracilis Neovagina – surgical scar
Do non-surgical options exist?
As mentioned above a non-surgical option does exist which is dilation therapy. According to many experts (including those from Boston Children’s hospital) the success rate of dilation is 95%. Dr Miklos & Moore feel this success rate is unsubstantiated as the definition of success is often based upon measurements instead of the ability of woman to have sex without discomfort or pain. In defense of dilation therapy, it is certainly the least invasive of all methods and has minimal complications.
Are vaginal dilators necessary after surgery?
The simple answer to this is it depends upon the surgical therapy one is utilizing. It is Dr Miklos & Moores experience that vaginal dilators are necessary during the healing process for: Davydov, Vecchietti, McIndoe as well as Gracilis Flap and not needed for Colon/Bowel Neovagina. However, this is strictly up to the surgeon making the recommendations. Once the vagina has become completely healed and matured and the woman is sexually active, she often will no longer need to dilate.
How long is the surgical recovery period of the Neovagina surgery?
Again, the answer to this depends on how one defines the recovery period. After the Davydov Neovagina the recovery required until intercourse is 12 weeks. After 12 weeks the patient can engage in intercourse without worry. Of course, with any surgical neovagina there maybe tenderness until the patient gets accustomed to her vagina.
Questions you should ask your surgeon prior to choosing to do a neovagina surgery?
- How many years have you been performing neovagina surgeries?
- How many neovagina surgeries have you performed during this time?
- What is the surgical success rate of this surgery in “your” hands? (not from some textbook or scientific paper)
- Why did you as a surgeon chose the neovagina surgical procedure you use? Most use the surgery they are taught which does not mean it is the best.
- How do you as a surgeon define success?
- When can I begin have sex?
- How big and how many incisions?
- What are “your” 3 most common intra operative complications when performing a neovagina surgery? And what percentage of “your” patients experience these?
- What are “your” 3 most common post-operative complications after performing a neovagina surgery and what percentage of “your” patients experience these”
- What is “your” average blood loss for your neovagina surgery? What percentage of your patients require a blood transfusion?
- How many neovaginas have you performed this year?
- Do you think it would be possible to speak with a neovagina patient of yours?
The potential neovagina patient should be careful when asking questions and accepting answers. Often surgeons will quote the literature and not their own statistics because they have so little experience. This is like saying you can shoot par on the golf course because PGA pros shoot par, or you can shoot 90% from the free throw line because an NBA pro can shoot that well. A surgeon should not tell just quote the literature but also if possible, their results based upon their skills.