
A 20-year-old MRKH patient from New York was diagnosed with MRKH (at 11 years of age) and had a successful Laparoscopic Davydov Neovagina procedure after previously failing a buccal mucosa neovagina performed 11 months earlier.
Her story begins at birth when she was born with a heart condition known as an atrial septal defect (ASD), which required two surgeries to correct. A few years later the patient began having recurrent lower urinary tract infections and was diagnosed with ureteral reflux and subsequently underwent surgery for prosthetic ureter valve and re-implantation. In 2008 she was diagnosed with poor kidney function and minor scoliosis. Finally, in 2011 she was diagnosed vaginal agenesis (lack of a vaginal canal), which is specifically known as MRKH.
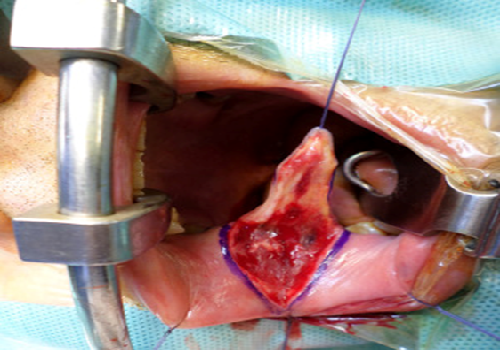
Patient was presented with the daunting task of trying to find the right doctor and correct treatment for her condition. This patient saw multiple doctors for her condition of vaginal agenesis in various states including: New York, Michigan, Pennsylvania, and Massachusetts. She attempted dilation for almost 2 years with minimal success. Finally, in 2019 she went to the University of Pittsburgh for an evaluation and was offered the surgery known as an Autologous Buccal Mucosa Neovagina. In this procedure, the skin on the inside of the patient’s mouth is harvested and essentially transferred to the vagina and sutured to lengthen the skin of the vagina. (Figure 1 and 2)

Our 20-year-old New York patient had the surgery performed and the surgeon measured the vagina at 8 cm. The patient was then required to spend 9 days in the hospital. One week later she needed to go back for a 2nd surgery to revise the vagina as it was noted that her vaginal length had already shrunk to 5 cm to which she could not place her dilator/mold. This patient unfortunately required a total of 3 surgeries at the University of Pittsburgh and within a matter of weeks was not able to place her dilators again due to the vaginal scarring and a short vagina.
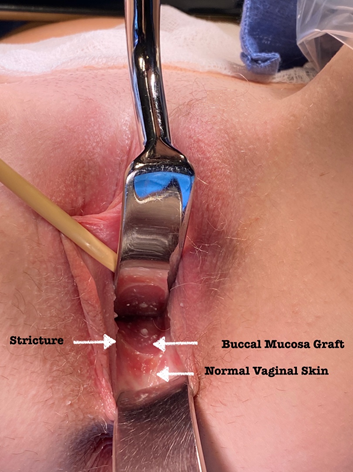
Frustrated with the results of her surgery this patient researched MRKH specialists and found Drs. Miklos & Moore in Atlanta, Georgia who offered her an alternative surgery i.e. the Laparoscopic Davydov Peritoneal Neovagina procedure. After a thorough evaluation and discussion, the patient decided to have the Laparoscopic Davydov Neovagina the next day after her physical consultation with Dr. John R. Miklos. During her physical consultation the patient’s vagina measured approximately 5 cm with a stricture at about 2.5 cm. A photo of the interior of her vagina reveals normal vaginal skin at the opening and the buccal mucosa extending more deeply into the vaginal canal (Figure 3). Notice the stricture/band of tightness between the two arrows demarcating her original short vaginal canal and the added buccal mucosa graft performed at the University of Pittsburgh.
This patient had the Laparoscopic Davydov Neovagina the next day after her physical consultation at Miklos & Moore Urogynecology and the surgery was subsequently performed within 2 hours, with a blood loss of less than a teaspoon and her vaginal canal was surgically lengthened to a total of 13 cm. It has been Drs. Miklos & Moore’s experience that 95% of surgical patients will likely shrink to an average size of 8-10 cm despite appropriate dilation. This, however, is the average size/length of the vaginal canal in women who have had a hysterectomy and greater than 95% of the time these patients can have pain free intercourse.
Drs. Miklos & Moore are honored and proud that this patient and her family trusted their experience, expertise and knowledge and pursued a laparoscopic Davydov Neovagina at their center after her failed buccal mucosa neovagina.
Drs. Miklos & Moore have performed over 600 of these surgeries since 1998 with outstanding success. At the completion of surgery 99% of all patients were given a vaginal length of > 9 cm.