This patient is a 61-year-old female with a chief complaint of chronic pelvic pain which all began after her TVT Advantage Sling (retropubic) insertion in 2010. (Figure 1) Initially she complained of tightness in her vagina, and then the pain got worse and she complained of pain down both her legs, specifically pointing to her medial thigh (i.e. adductor region).
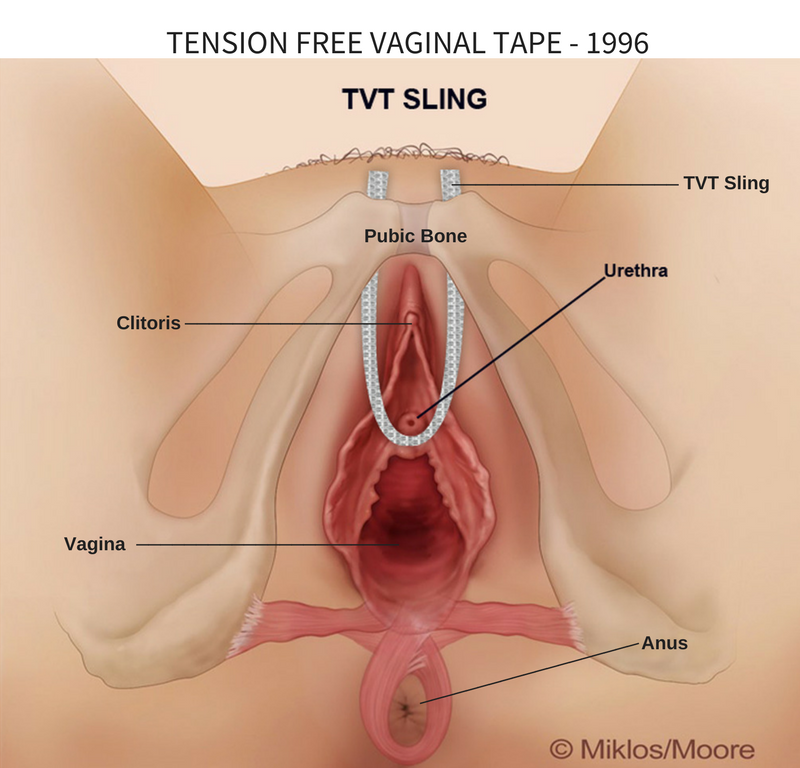
Figure 1: Normal placement of TVT retropubic sling. A transvaginal approach to mesh removal will usually result in 5-6 cm of mesh removed, whereas using a laparoscopic and vaginal approach can result in complete removal of 15-24 cm. 1996 was the year TVT was introduced in Europe.
After much research, in 2013, the patient decided to see a world leader in mesh removal at UCLA. Specifically, she saw the director of female urology and female pelvic medicine in the department of urology. She was told that he could remove all of her TVT retropubic mesh through a vaginal incision. After the surgery, the doctor admitted he could remove some but not all the TVT mesh due to severe scar tissue on the back of the pubic bone. She was readmitted to the hospital 24 hours later for a blood transfusion but did claim some pain improvement. She was taken back for a second surgery (2014) to have a 4 corner RAZ procedure (Figure 2) for a cystocele and recurrent cough leakage.
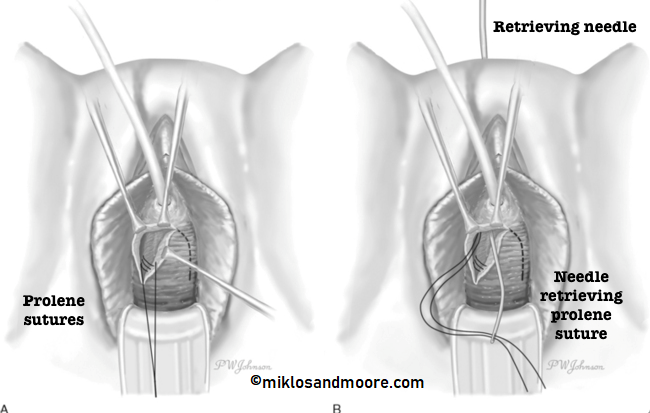
Figure 2: 4 Corner Raz Procedure — is performed to lift the bladder and the urethra to treat a cystocele and cough leakage. The surgery is performed by using 4 prolene sutures which are stitched into the supportive tissue of the urethra and bladder from a vaginal approach and then passed to the abdominal wall just like a TVT sling. Here we see the passage of 2 sutures and in the 2nd illustration a needle from the pubic area being passed through the vagina to retrieve the sutures.
The patient came to see Drs. Miklos & Moore to see if the rest of the sling mesh could be removed. The examination of this patient revealed 10/10 pain in the bladder and urethra. This patient felt her condition was severe enough that she wanted to remove the rest of the sling. Dr. Miklos explained in her situation the second surgery performed i.e. the RAZ procedure (prolene sutures) should also be removed because it was in the same area as the original TVT advantage sling and was anchored (through scar tissue) to muscle and fascia layers. The muscle and fascia are the layers of most pain. This surgery was performed doing both a vaginal and laparoscopic approach. (Figure 3)
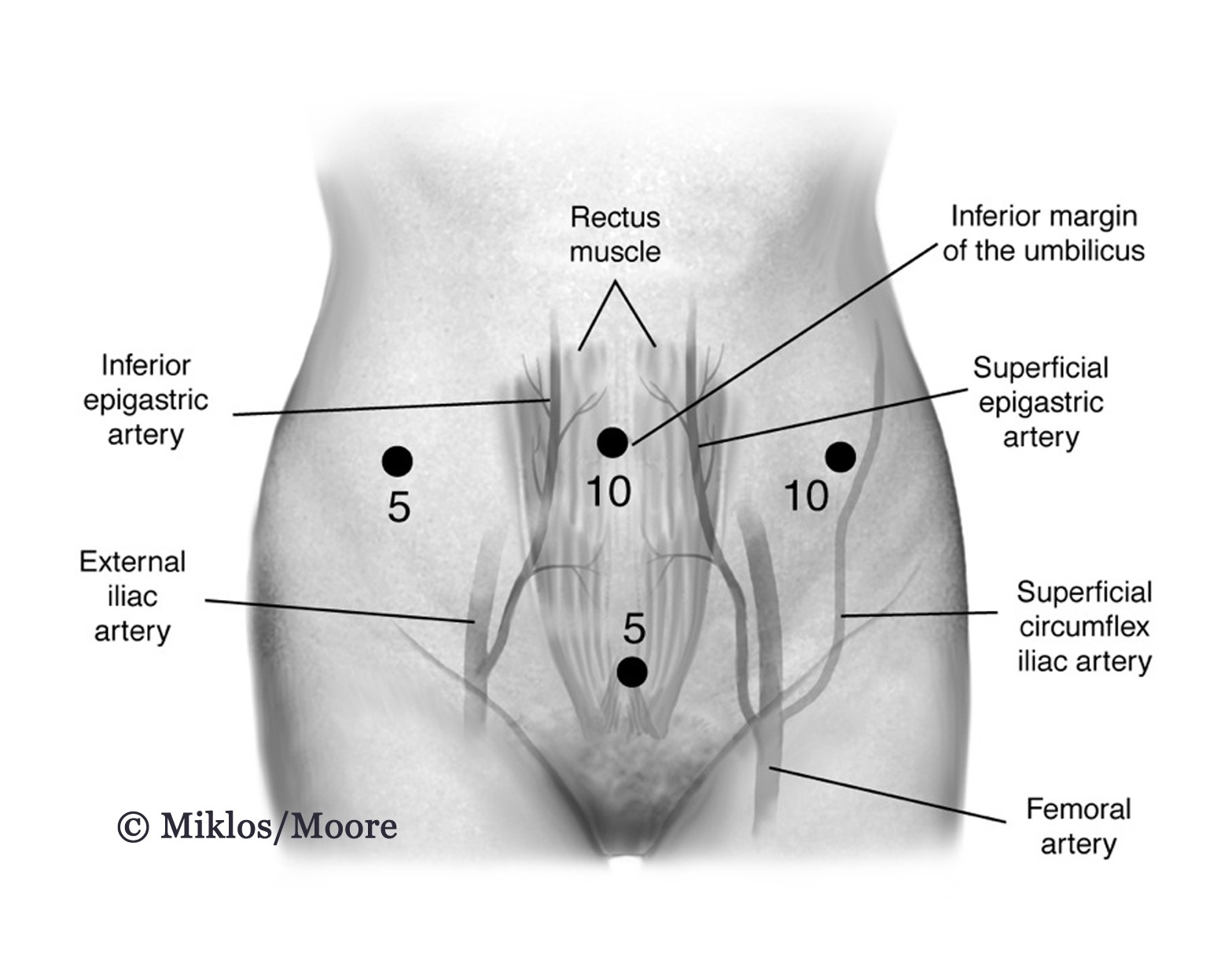
Figure 3 – Laparoscopic approach is required to remove the whole TVT sling, it is impossible to remove the whole TVT through a vaginal approach.
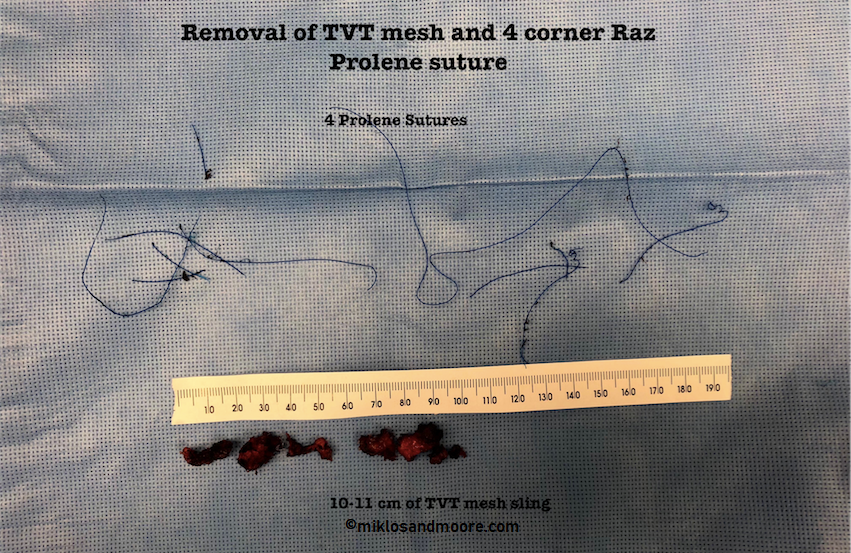
Drs. Miklos & Moore explain it is impossible to remove the whole sling through a vaginal incision, contrary to what is said at UCLA or other institutions. The average length of mesh placed at the time of a TVT retropubic sling is approximately 16-24 cm. Drs. Miklos & Moore removed all four Prolene sutures (RAZ procedure) and the remainder of the TVT Advantage mesh. (Figure 4)
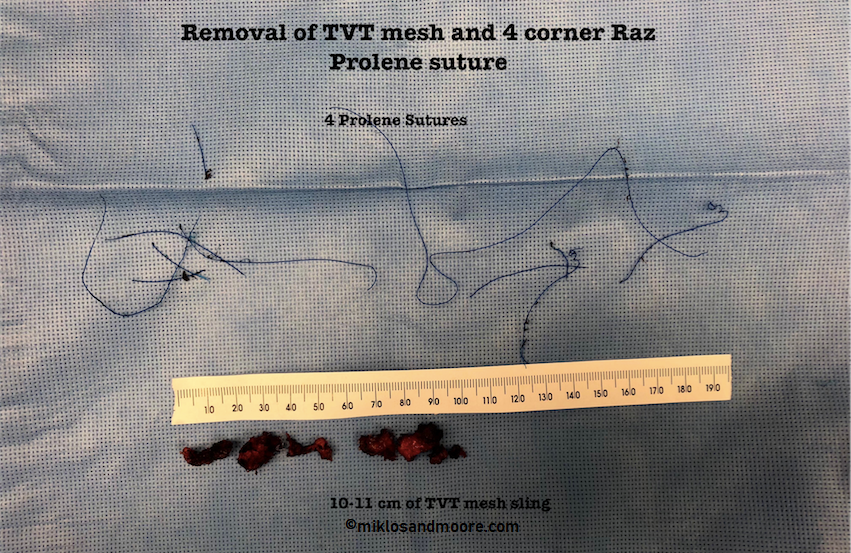
Figure 4: Removal of the remaining 10 cm of TVT Advantage mesh and all 4 Prolene sutures of the 4 Corner Raz procedure, which requires a laparoscopic approach.
Miklos & Moore Words of Wisdom:
- TVT slings cannot be completely removed through a vaginal incision. If a surgeon’s states that they can be, they are either ignorant or not being truthful.
- Only approximately 1/3 of the sling can be removed from a vaginal approach.
- TVT slings do not always need to be completely removed. If the patient only has vaginal pain then a vaginal approach is all that is often required.