
WHAT ARE THE SIGNS AND SYMPTOMS OF A FAILED TOT SLING?
The TOT (trans obturator tape) mesh sling is made to treat stress urine incontinence i.e., SUI. If one places a TOT sling and it doesn’t correct the SUI, then that would be considered a failure. The patient would feel leakage with coughing and sneezing and the healthcare professional could see the leakage during an exam.
A failed TOT sling may also mean that the patient no longer has urinary incontinence however the patient suffers from a complication which affects one’s quality of life. What good is a surgery if it corrects the urine leakage but leaves you with a complication which affects your quality of life. The most common complications associated with a TOT sling are as follows:
Chronic Pain– is one of the most common & most devastating complications of transvaginal mesh surgery. This can be caused by nerve damage, mesh erosion into neighboring organs (such as the bladder or urethra), or pulling on the nerves of the groin, legs and/or pelvis. Pain is most commonly due to excessive scar tissue, produced by the interaction of the human body to the mesh, which can pull on nerves resulting in pain.
Groin Pain- is also a common problem as the mesh continues to scar and tighten this will pull on the obturator nerves which supply the inner thigh and the groin. There are few conditions in the world that give groin pain. If a patient has groin pain and the pain increases with abduction of her legs (spreading her legs apart), there is a very good chance the TOT sling is the culprit.
Painful sex – the mesh can cause painful intercourse for the patient and / or her partner. Again, mesh stimulates scar tissue formation which in turn can cause pain by creating tension on the nerves or simply be the mesh exposure, extrusion, or erosion of mesh.
Infections – can occur due to the continuous irritation of the mesh on the neighboring tissue or organs. Symptoms of an infection may include: pain, fever, or vaginal discharge.
Mesh exposure -transvaginal mesh can become exposed, thus one can actually see the mesh coming through the vaginal skin, but it does NOT protrude beyond the height of the skin. This can produce pain or painful intercourse for the patient and/or her partner as well as bleeding and infection.
Mesh extrusion – the mesh is not only exposed through the skin but is protruding above or beyond the borders of the skin. Mesh extrusion can have all the symptoms of mesh exposure or erosion.
Mesh erosion – is like mesh exposure however instead of the mesh migrating or being seen on the outside i.e., as a disruption in the skin of the vagina one would see the mesh penetrating the inside of a neighboring organ such as the urethra, bladder, or rectum. When this happens common signs or symptoms include pain, bleeding, infection, painful intercourse or potentially blood in the urine or in the feces as well as pain during urination or defecation.
Urinary problems – may include complete urine retention, the inability to empty one’s bladder, urgency, frequency, overactive bladder, recurrent urinary tract infections or urinary incontinence. The mesh can cause urinary problems, such as urinary incontinence, urinary retention, and urinary tract infections.
If you are experiencing any of these signs or symptoms after undergoing mesh surgery, it is important to consult with an experienced mesh removal surgeon or healthcare provider for proper evaluation and treatment. All too often patients are having mesh failures inappropriately evaluated or even treated. Failure to remove the mesh appropriately can lead to further complications and worsening conditions as well as making the remainder of the mesh even more difficult to find and remove in future surgery.
WHY CHOOSE MIKLOS & MOORE UROGYNECOLOGY TO REPAIR YOUR FAILED TOT SLING?
Dr. Miklos is a highly experienced and skilled surgeon who specializes in the treatment of mesh complications. He has removed more than 1,000 pieces of mesh and has been removing mesh since 1994. Few surgeons in the world can make this claim. Dr. Miklos has a patient-centered approach to care and he listens to the patient’s point of view which is not always supported by the scientific literature. He takes the time to thoroughly evaluate each patient’s unique situation and then develops a personalized treatment plan for each patient. Dr. Miklos makes recommendations but allows each patient to make the final decision as to the surgery and technique. He truly believes that he makes the patient an informed consumer so she can ultimately make the right decision to minimize or stop the patients’ pain and suffering. Overall, choosing Dr. Miklos for your mesh complication surgery can provide you with the expert care and support you need to achieve the best possible outcome. Dr Miklos has:
EXPERIENCE -First and foremost at Miklos & Moore Urogynecology the doctors listen. They have been removing mesh since 1994 and have seen, treated, or removed just about every type of transvaginal mesh complication known to man. They have removed more than 1000 pieces of mesh with minimal complications and superior success. They have written the largest paper on sling removal in the world and represents the second largest series of patients having the total TOT sling removed from the vagina and groin. Dr Miklos has removed more than 150 total TOT slings which requires a vaginal incision as well as two groin incisions. (Figure 1-3)
EXPERTISE – Dr. Miklos has treated patients from all over the world for mesh complications. Miklos & Moore Urogynecology has produced award winning videos which have gotten them international acclaim for their mesh removing techniques. Dr. Miklos has taught post graduate courses for mesh removal at conferences in the USA, South Africa, Europe, and the UK.
KNOWLEDGE – Drs. Miklos & Moore are Rule 26 medical legal experts who understand the law and malpractice cases facing patients today. They are also leaders in the world on mesh complications as they have written some of the largest papers on mesh complications found in the worldwide literature.
RESULTS – Miklos & Moore Urogynecology have addressed and removed some of the most difficult transvaginal mesh devices made and inserted in the human body. Though no one can guarantee the success rate for fixing the patients symptoms, Dr Miklos can usually remove >95% of the mesh load > 90% of the time. He can totally remove the complete TOT sling implant most of the time if it is indicated.
Here at Miklos & Moore Urogynecology we have removed approximately 150 total TOT slings. This means the total or whole TOT has been removed from the body. In one patient alone he removed a total of 6 arms or 3 total TOT slings.

Figure 1
TOT under urethra

Figure 2
TOT in left groin
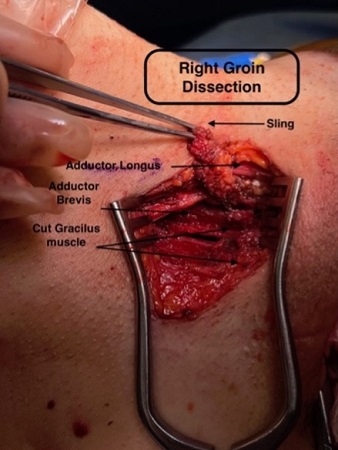
Figure 3
TOT right groin
RECOVERY TIME AFTER FAILED TOT SLING REMOVAL SURGERY
The recovery time after failed TOT sling removal surgery depends upon the actual surgical procedure performed as described above. We can essentially categorize the recovery based upon 3 different types or techniques of TOT sling removal (SEE Medical Illustration below)
- Transvaginal sling incision partial removal. These patients have a minimal amount of mesh sling removed and this is accomplished through one transvaginal incision of 2 cm. This incision is made under the urethra to gain exposure to the implanted mesh. After the mesh is either cut or removed through this 2 cm vaginal incision, a suture is used to close the incision. Usually, the TOT mesh sling is cut or partially removed for complications such as urine retention or painful intercourse at the urethra. This procedure can be done as an outpatient and there is usually very little pain involved. The patients can return to work the next day but are restricted from intercourse for 4 weeks. Usually they are pain free in 1-2 days.
- Total TOT removal – requires a transvaginal sling incision and removal via the vagina then an inguinal or groin incisions to remove the TOT arms which penetrate the obturator membrane, muscles and adductor muscles. With a total TOT removal, the patients usually spend one night in the hospital and can go back to full normal activity in 6 weeks. If the patient happens to get a concurrent laparoscopic (non-mesh) Burch for SUI to replace the sling, then the patient is restricted from heavy lifting or intercourse for 12 weeks. Usually with a total TOT removal the patient is pain free in 1-2 weeks.
- TOT removal from the urethra or bladder. These patients also spend one night in the hospital and can go home the next day. We recommend 6 weeks of no sex or heavy lifting or straining until the vaginal, inguinal or abdominal incisions heal. The patient may require a fukk 12 weeks of healing if the patient decides to receive a non-mesh anti leakage operation such as a Burch. Most patients are usually pain free in 1-2 weeks.
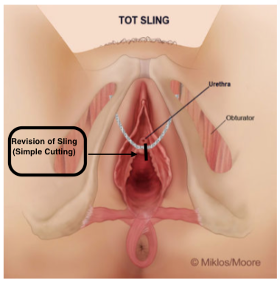
Figure 4
TOT cutting for urine retention
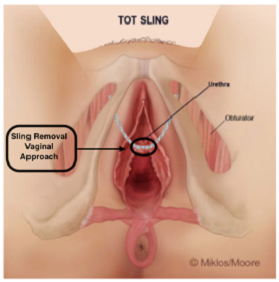
Figure 5
TOT partial removal
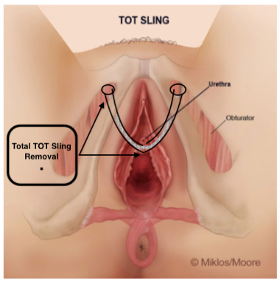
Figure 6
Total TOT removal
Posterior Vaginal Mesh Removal