

TVT Sling and Vaginal Pain
Tension-free vaginal tape ie TVT slings whether retropubic, obturator (aka TOT) or single incision (aka mini slings) can all cause complications such as vaginal pain and painful intercourse. However, it is often difficult getting to get the physician or surgeon to understand or diagnose the problem. Industry, doctors, surgeons and key opinion leaders in the field of Urology and Urogynecology refuse to believe that synthetic or non-synthetic sling procedures can result in complications such as vaginal pain, pelvic pain, painful intercourse (aka dyspareunia), lower abdominal pain as well as groin and leg pain.
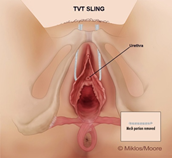
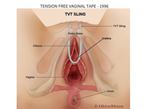 TVT –retropubic |
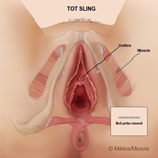
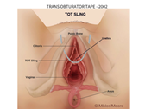 TVT – obturator |
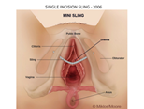 TVT-single incision sling |
Often patients do not know which slings they have had placed and sometimes knowing the time line as to the introduction of these slings into the U.S. is helpful. The TVT sling ie retropubic sling was introduced into the U.S. in 1998, the TVT-O was the second-generation sling which attempted to reduce intraoperative complications such as bladder and bowel injuries was introduced in 2002 and finally the single incision sling (aka SIS or mini sling) was introduced in 2006. As you may or may not be aware there are many different companies which make these slings and all have various nuances of structure and delivery systems but essentially, they follow the same pathways of delivery, made of the same material polypropylene and have the same mechanism of action to treat urine incontinence.
Often patients will complain of pain after receiving one of the TVT type slings and most commonly the pain is isolated to the vagina and is exacerbated with intercourse. This pain was not present prior to sling placement but manifested after the insertion of the sling. It does not take a rocket scientist to propose that most likely the pain is caused by the surgical procedure or the actual sling itself. Patients can have pain with or without intercourse. If the patient states I have vaginal pain all the time, since the placement of the sling, of course that surgery and sling is suspect but it is not diagnostic. If the patient states I have pain with penile insertion and thrusting this also adds to the history the sling might be the culprit or the origin of her pain. Though taking a history is very important it is just a piece of the puzzle and may not be completely reliable in determining whether the sling causes pain. Many surgeons suggest an MRI, CT scans and Ultrasounds these radiologic tests are rarely helpful in the diagnosis of pain and no patient needs to be told by an machine that she has pain. Even more important than a history or radiologic test is the examination as this will often locate and reproduce the point of pain during simple touching aka palpation. Pain usually present in two areas: 1) in the vagina alone or 2) along the sling pathway where it has been placed. The pain in the vagina is the pain which is most reproducible during an exam.
Vaginal pain is best determined by an examination in combination with taking a woman’s history. One way of determining whether the sling is causing vaginal pain is to examine the patient without the patient knowing exactly what area of the vagina the surgeon is touching. Drs Miklos & Moore do what is called a blind visual pain analog scale (VPAS) test. This means the patient is looking at a VPAS scale while different areas of the vagina (where the sling is and is not) are palpated and the patient is asked if they have pain and the amount of pain they feel. Dr Miklos & Moore usually palpate 11 different areas of the vagina during the exam but do not tell the patient if they are touching the sling.
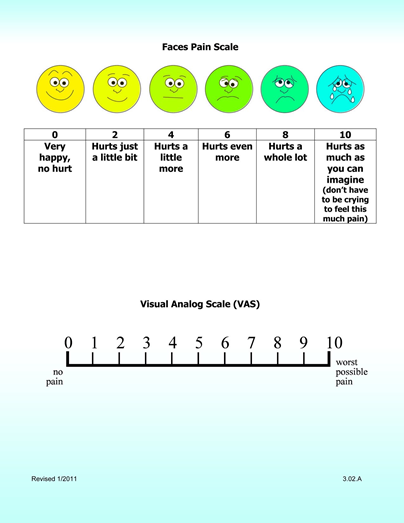
Visual Pain Analog Scale
Patients who have vaginal pain due to the sling will declare that the highest amount of pain is along the pathway of the sling. Pain will be especially prominent at the lateral areas just before insertion into the muscle and fascia layers. It has been Drs Miklos & Moore experience that the pain is lessened directly under the urethra where the sling is flatter and does not have as much tension as compared to sling extending lateral to the urethra. It is not unusual for the patient to say she has a zero 0/10 pain directly underneath the urethra and a 10/10 pain lateral to the urethra where the sling is taut and stretched. If the sling is palpated, especially lateral to the urethra, and the patient states this does not cause pain then there is a greater likelihood the sling is not reason for her pain. Drs Miklos & Moore examination technique is not utilized to trick the patient but instead reduce the chance of taking a patient to surgery for the unnecessary removal of the sling. They want to make sure the patient is indeed suffering from pain due to the sling.
If the pain is isolated to the vagina with or without intercourse the best treatment for the pain is a transvaginal removal of the sling and this usually results in removing approximately 5-6 cm of mesh (2.54 cm = 1 inch). Most surgeons will just cut the sling or remove a few millimeters and this does not usually take the tension off the mesh. Drs Miklos and Moore experience has shown them that removing the maximum amount of mesh has the greatest chance of helping the patients vaginal pain or painful intercourse.
 TVT sling pain |
 TVT – O Obturator sling |
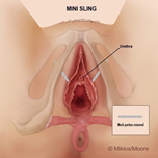 Single Incision Sling Vaginal Portion Removed |
In the hands of Drs Miklos and Moore removal of the vaginal portion of the sling for vaginal pain and painful intercourse is a very safe and effective operation. They estimate that if the patient has not pain only with intercourse removing the vaginal portion of the sling will fix the pain with sex in >90% of patients. If the patient has pain and tension in the vagina all the time ie with or without intercourse removing the vaginal portion of the sling seems to reduce or cure pain approximately 70% of the time. There is no way of knowing if the removal of the sling will cure the pain unless one removes the sling.
|
TVT retropubic |
TVT – O Obturator (TOT) |
Single Incision Sling |
If the patient is suffering from pain in other areas of the pelvic floor such as the lower abdomen, pubic area, legs or groin then those areas will also be addressed. Complete removal of these slings is much more complicated and require a significantly more skill and time to remove the whole sling. Drs Miklos and Moore have written one of the world’s largest papers on synthetic mesh sling removal (please click here to read). Often patients suffering from pain in these areas have much more debilitating and devastating pain. In patients suffering with these conditions I suggest you refer to the blog on complete TVT sling removal. In these situations, a harder, much more complex surgical procedure is required for each type of these sling procedures ie TVT retropubic, TVT obturator and TVT single incision sling.
If you require need to be evaluated for vaginal, groin, lower abdominal pain and you think it is due to a synthetic TVT, TOT or single incision sling contact a surgeon who is knowledgeable about complete vaginal removal or total removal of the transvaginal mesh slings.