
MRKH TREATMENT OPTIONS
There are excellent treatment options available to create a functioning vagina. Some older techniques are much more invasive than others and require large abdominal incisions with major surgery, extensive recovery and very large abdominal wall scars while others require skin grafts, muscle flaps taken from the legs or other areas which are also very invasive with extensive recovery time. Drs. Miklos and Moore utilize a modification of an abdominal technique that utilizes the patient’s own peritoneum, requires no grafts or implants and has excellent success rates, however they utilize a laparoscopic approach with mini-incisions that enables the procedure to be completed on an outpatient basis with a very rapid recovery.
MRKH SURGICAL TREATMENT OPTIONS
Patients with vaginal agenesis will need treatment to become sexually active and therefore will need the creation of a neovagina. MRKH surgery is only required if the patient desires to have intercourse and can only be decided upon by the patient after becoming an informed consumer. Timing of this will depend on the patient and her family and the surgeon feel she is emotionally and physically mature enough to undergo the procedure or surgery. Ideally, in the past it was felt that the patient should be ready to be sexually active shortly after any surgical procedure to create a vagina, however many patients and families opt for treatment prior to this as the young woman desires a vaginal canal at a younger age as she wants to feel “normal” and doesn’t want to wait until she is ready to be active. This is certainly understandable and why many young women undergo the procedure in their late teens. In this case, if the young woman is not planning on sexual activity for a period (and this could be years) after the surgery, then she will need to be prepared to use dilators to maintain the vaginal canal until she is having intercourse on a regular basis.
There are excellent surgical treatment options available to create a functioning vagina. Some older techniques are much more invasive than others and require large abdominal incisions with major surgery, extensive recovery and very large abdominal wall scars while others require skin grafts, muscle flaps taken from the legs or other areas which are also very invasive with extensive recovery time. Drs. Miklos and Moore utilize a modification of an abdominal technique that utilizes the patient’s own peritoneum, requires no grafts or implants and has excellent success rates, however they utilize a laparoscopic approach with mini-incisions that enables the procedure to be completed on an outpatient basis with a very rapid recovery
Other Treatment Options (Non-Surgical) include:
Do Nothing
The decision to engage in surgery is a personal decision for each patient. Only the patient can make the final decision if they want to consider neovagina surgery. There are many woman with MRKH who do feel that a vagina nor surgery is not necessary to engage in intimacy and for those women their decision is the correct choice. Many of women also do not feel the need or desire to engage in non-surgical treatment ie self-dilation. Again, this is the right decision for that woman. Still most women have the desire to attain a functional full length vagina and they too are making the correct decision for their lifestyle and their bodies.
Non-surgical Neovaginal Treatment Intermittent Pressure (aka Frank Method)
The Frank method was named after the doctor who first introduced this technique in the 1930’s. Dilation is sometimes used as a first attempt to create or lengthen the very short or non-existent vagina. In this treatment, the patient presses (or eventually sits on) a small rod (dilator) against the skin or the small vagina for 15-20 minutes a day. Progressively larger dilators are used to expand and lengthen the vagina. Several months may be required to obtain the needed length. It is recommended that the vagina be at least 2.5 cm in length to start (i.e. prior to dilating) otherwise the success rates are often disappointing. Ingram (1981) reported a 77% “favorable “experience in 26 patients.
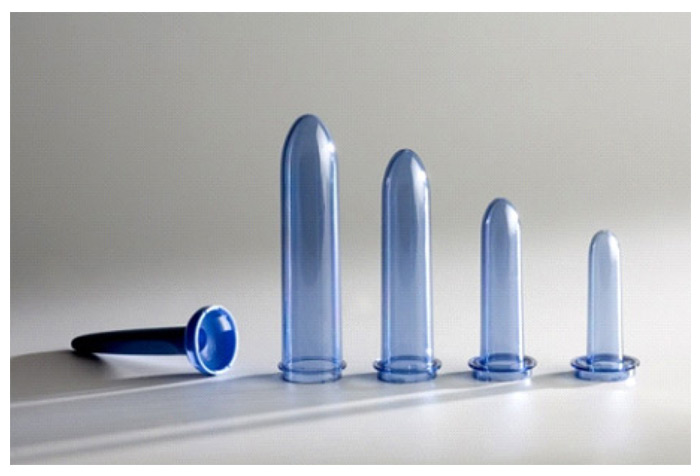
Modern Dilators
In the 1990’s the rod-shaped dilators were attached to a firm base so the patient could sit on the dilator and use the pressure of her body exerted against a hard chair to stretch the vagina in length and width. This advancement was simple yet important it allows the woman to adjust pressure by lifting and settling her body on the dilator. The design allows for small incremental adjustments of the dilators to lessen the discomfort with each successive dilator. This alone increases a patients’ compliance.
Please note the word dilation may not be the best verbiage for what the patient is really trying to accomplish. What the patient is hoping to accomplish is vaginal lengthening and dilation but really lengthening is the ultimate goal.
Dilators with Removable Handle

Conical Dilators

Dilators with a Base