

Failed Mesh Removal at Duke University.
This patient was a 57-year-old patient that came to us with the following chief complaints: 1) vaginal pain 2) urethral pain and 3) right groin and right hip pain that goes from the deep groin all the way to the buttocks. She had the original TOT sling (Figure 1) and the anterior Avaulta Mesh (Figure 2) for treatment of stress urinary incontinence, as well as a cystocele by her gynecologist in 2008.
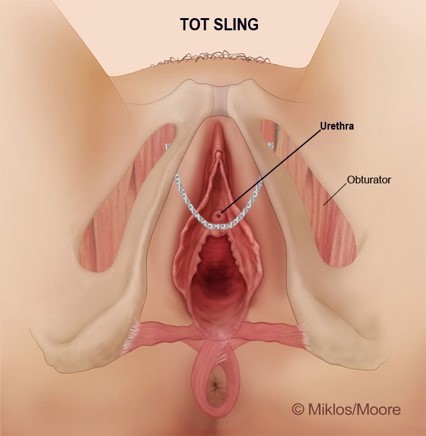
Figure 1
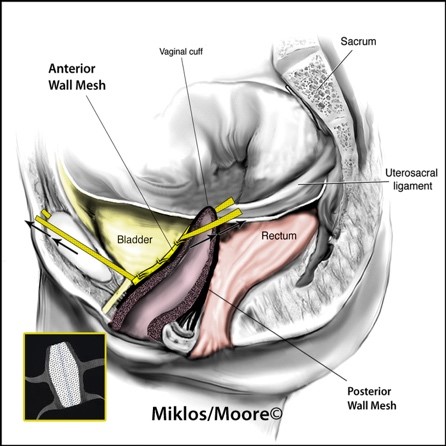
Figure 2
This patient underwent a total of 12 revision/removal mesh surgeries when she only needed one. She had two in office revisions by the implanting surgeon and then taken to the operating room for removal of extruding mesh in 2009. She claims she sought help by urogynecologists at Duke University where she underwent 8 more surgeries in the operating room (according to the patient).
She offered that she feels the problem is the anterior Avaulta Mesh and that the TOT Sling was not a problem. She claims that only one time was the surgery performed for mesh extruding through the skin. All surgeries performed at Duke were performed for pain and most of these surgeries entailed only cutting the mesh to remove the tension on the mesh. Her last two surgeries were performed laparoscopically (on 3/2013) and then robotically (on 4/2013). On the final surgery, a total of 3.5 cm x .7 cm fragment (Total = 2.45 square cm) had been removed. She states this did not fix or help her pain.
Please note per Dr. Miklos: it is impossible to remove the complete anterior vaginal wall mesh laparoscopically or robotically. The safest, most effective and most efficient way to remove the mesh is via a vaginal approach.
The patient sought Drs. Miklos & Moore for their experience in transvaginal mesh removal. Dr. Miklos explained that he could remove all the mesh in the vagina but did not feel it was appropriate to remove the arms of the mesh in her groin based upon his clinical findings. She went to the operating room where Dr. Miklos removed 6 cm x 1.0 cm (total of 6 square cm) of TOT sling mesh (Figure 3) and then removed the whole vaginal portion of the anterior wall mesh which measured approximately 10 cm x 4 cm (total of 21 square cm). (Figure 4)
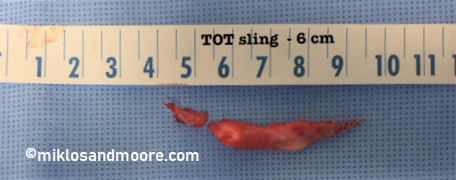
Figure 3 – TOT Sling

Figure 4 – Anterior Avaulta
Drs. Miklos & Moore removed approximately 27 square centimeters of mesh which is 11 times the amount of mesh removed by Duke University. (27 cm2 versus 2.45 cm2). Drs. Miklos & Moore removed all of the mesh present in the anterior vaginal wall, both the Avaulta and the TOT sling. Postoperatively the patient claims her pain was gone in the urethral area and the pain persisted but was initially less intense in the rest of the vagina and the pelvic regions.
This patient is NOT cured of her symptoms and she may never be cured. It has been Drs. Miklos & Moore’s experience that early removal of mesh is imperative when one is suffering from pelvic, vaginal, bladder, urethra, groin and lower abdominal pain. The longer the mesh is in place the greater amount of inflammation, scar formation and contraction of the mesh, which can, in turn, cause pain or worsen the pain. Prolonged contracture on muscles and nerve can cause permanent nerve damage and permanent pain.
This patient underwent over 11 removal or revision surgical procedures because the doctors addressing her condition were not well trained in mesh removal. They should have removed all the mesh through a vaginal approach, as this patient did not need a laparoscopic or robotic surgery to remove the mesh. She underwent many needless surgeries. Please choose a surgeon with experience, expertise and one who can remove mesh. Do not choose an institution, but instead choose a surgeon who has the experience.
Drs. Miklos & Moore: Pearls of Wisdom
- Patients suffering from pelvic, vaginal, groin, lower abdominal pain at rest should have their mesh removed in total (if possible) sooner rather than later. Waiting can result in permanent pain.
- Patients who have pain only with sex have a better chance of surgical success than those who suffer from pain all the time.
- Cutting the mesh without removal usually will not lessen or not stop the pain.
- When pain is chronic and constant consider removing all the mesh if possible.
- Anterior vaginal wall mesh and TOT slings cannot be removed through an abdominal incision (laparoscopic, laparotomy or robotically) It is IMPOSSIBLE!!!